Women who follow seven healthy habits might lower their risk of developing dementia, according to new research presented at the American Academy of Neurology’s 75th Annual Meeting this week.
In their study, researchers followed 13,720 women for 20 years to analyze their risk of developing dementia. They examined Medicare claims at the end of the study to determine who received a diagnosis.
The women received a score for seven health factors, with 0 corresponding to “poor” and 7 as “excellent.” The average score at the beginning of the study was 4.3. At the 10-year follow-up, it was 4.2.
At the 20-year follow-up, 1,771 women had been diagnosed with dementia.
After adjusting for factors such as age and education, the researchers found that for every increase of one point in overall score, the participant’s risk of dementia decreased by 6%.
One limitation of the study is that researchers did not receive information that allowed them to see how changes in healthy habits, such as quitting smoking, influenced the risk of dementia.
The findings also have not been published yet in a peer-reviewed journal.
The 7 health lifestyle habits
The researchers used the American Heart Association’s “Life’s Simple 7”Trusted Source lifestyle habits for their study.
Those seven factors are:
Being active
Eating better
Maintaining a healthy weight
Not smoking
Maintaining healthy blood pressure
Controlling cholesterol
Having low blood sugar
“The good news is, this isn’t an all-or-nothing situation,” said Dr. Joel Salinas, a behavioral neurologist and researcher at NYU Langone Health and chief medical officer at Isaac Health in New York.
“You don’t need to be the healthiest person. Even if people have a good score in one or two areas, they are receiving some benefit. Any improvements incrementally improve your long-term health,” he told Healthline.
“If you change your habits, you will receive some health benefits. The earlier you make those changes,” Salinas added. “The longer you keep the new habits, the better. The intent is to find an easy way to keep track of your health.”
What is dementia?
“Dementia is an overall decline in cognitive ability, usually impacting short-term memory (learning/recall new information) and another cognitive ability (or more), such as decline in executive skills (organization, decision making) or language, or visual-spatial skills,” says Karen Miller PhD, a neuropsychologist and geropsychologist as well as the senior director of the Brain Wellness and Lifestyle Programs at Pacific Neuroscience Institute in California.
“In dementia, these declines typically impact one’s ability to be completely independent (i.e., the person may have difficulty managing finances or medications, difficulty/impairment in driving, etc.),” she told Healthline.
Women make up about two-thirds of people with dementia, including Alzheimer’s disease, according to a 2021 reportTrusted Source.
One reason is that women live longer than men and dementia typically appears after age 80. Other possible explanations, according to Cognitive Vitality, a program of the Alzheimer’s Drug Discovery Foundation, include:
Higher education is associated with lower rates of dementia. Many older women today were not afforded the same educational opportunities as men.
Dementia is linked to depression, and more women have depression than men
People who exercise are less likely to develop dementia and women exercise less than men
When women develop dementia, they decline faster than men do. Therefore, they can have a more severe illness.
Dementia occurs when neurons in the brain stop working or interacting with other brain cells, according to the National Institute of AgingTrusted Source.
Everyone loses some neurons as they age, but people with dementia have a more significant loss.
While many people over 85 have dementia, it is not considered a normal part of aging.
Types, symptoms of dementia
Alzheimer’s disease is the most common form of dementia, but it is not the only one.
A few other types of dementia include the following:
Frontotemporal dementia
Lewy body dementia
Vascular dementia
Some people can have a combination of two or more types of dementia.
Signs and symptoms of dementia include:
Experiencing memory loss, poor judgment, and confusion.
Difficulty speaking, understanding, and expressing thoughts, or reading and writing.
Wandering and getting lost in a familiar neighborhood.
Trouble handling money responsibly and paying bills.
Repeating questions.
Using unusual words to refer to everyday objects.
Taking longer to complete routine daily tasks.
Losing interest in normal daily activities or events.
Hallucinating or experiencing delusions or paranoia.
Acting impulsively.
Losing balance and problems with movement
It is important to note when symptoms are worsening, experts say.
“When people start noticing these symptoms, in themselves or a loved one, it may be time to see a doctor. The same is true for new changes, new symptoms, or a worsening of previous symptoms. There are some treatments – that can’t cure or reverse the damage. Still, they can possibly slow the progression of the disease, such as aducanumab and lecanemab,” Salinas said. “New treatments are another reason to see a doctor.”
Source: Healthline.com
DISCLAIMER: Independentghana.com will not be liable for any inaccuracies contained in this article. The views expressed in the article are solely those of the author’s, and do not reflect those of The Independent Ghana
After receiving a diagnosis of aphasia, which affects speech and language, the actor, 67, ended his 40-year career in March.
His ex-wife Demi Moore, wife Emma Heming Willis, daughters Rumer, Scout, Tallulah, Mabel, and Evelyn have all released a joint statement on Instagram providing “an update” on his health.
“Our family wanted to start by expressing our deepest gratitude for the incredible outpouring of love, support, and wonderful stories we have all received since sharing Bruce’s original diagnosis,” the caption reads.
“In the spirit of that, we wanted to give you an update about our beloved husband, father and friend since we now have a deeper understanding of what he is experiencing.
“Since we announced Bruce’s diagnosis of aphasia in spring 2022, Bruce’s condition has progressed and we now have a more specific diagnosis: frontotemporal dementia (known as FTD).
“Unfortunately, challenges with communication are just one symptom of the disease Bruce faces.” “While this is painful, it is a relief to finally have a clear diagnosis.”
The family also explained on the Association for Frontotemporal Degeneration website, “FTD is a cruel disease that many of us have never heard of and can strike anyone. For people under 60, FTD is the most common form of dementia, and because getting the diagnosis can take years, FTD is likely much more prevalent than we know.
“Today there are no treatments for the disease, a reality that we hope can change in the years ahead.”
With them keen to “shine a light on this disease”, here’s what we know about the signs and symptoms of different types of dementia, including frontotemporal.
Watch: Bruce Willis diagnosed with frontotemporal dementia
What is dementia?
Dementia is a syndrome (a group of related symptoms) associated with an ongoing decline of brain function, according to the NHS. There are many different types, with many different causes, and it is not a natural part of ageing.
For example, Alzheimer’s disease and vascular dementia are two different types, with both of them making up the majority of cases. Other types include frontotemporal dementia, dementia with Lewy bodies (DLB), young-onset, as well as mixed dementia (more than one at the same time).
The condition can affect memory, as well as the way you speak, think, feel and behave.
There are currently around 900,000 people with dementia in the UK, projected to rise to 1.6 million by 2040, according to the Alzheimer’s Society.
The likelihood of developing dementia increases significantly with age. One in 14 people aged over 65 has the condition, which rises to one in six for those aged over 80. However, it can affect younger people too.
Alzheimer’s disease
The first signs of Alzheimer’s disease are usually minor memory problems. (Getty Images)
Alzheimer’s disease is the most common cause of dementia in the UK. It is a progressive condition, meaning symptoms develop gradually over many years, slowly becoming more severe.
The exact cause isn’t yet fully understood, though factors that can potentially increase your risk include age, a family history, untreated depression and lifestyle factors associated with cardiovascular disease.
The first sign is usually minor memory problems, such as forgetting about recent conversations or events, or forgetting the names of places and objects.
As the condition develops and symptoms become more severe, as listed by the NHS, these include:
Confusion, disorientation and getting lost in familiar places
Difficulty planning or making decisions
Problems with speech and language
Problems moving around without assistance or performing self-care tasks
Personality changes, such as becoming aggressive, demanding and suspicious of others
Hallucinations (seeing or hearing things that are not there) and delusions (believing things that are untrue)
Low mood or anxiety
Vascular dementia
Vascular dementia can make you feel disorientated. (Getty Images)
Symptoms of Alzheimer’s disease, such as problems with memory and language (many people with vascular dementia also have Alzheimer’s disease)
This can make daily life increasingly hard for someone with the condition, eventually preventing them from being able to look after themselves.
Dementia with Lewy bodies (DLB)
DLB can make you feel sleepy or disturb your sleep. (Getty Images)
DLB, also known as Lewy body dementia, is another common type of dementia. It is caused by the Lewy bodies, which are clumps of protein that appear in the nerve cells of the brain. As it shares symptoms with Alzheimer’s disease and Parkinson’s disease, it is often wrongly diagnosed.
Symptoms listed by the NHS include:
Hallucinations – seeing, hearing or smelling things that are not there
Problems with understanding, thinking, memory and judgement – this is similar to Alzheimer’s disease, although memory may be less affected in people with dementia with Lewy bodies
Confusion or sleepiness – this can change over minutes or hours
Slow movement, stiff limbs and tremors (uncontrollable shaking)
Disturbed sleep, often with violent movements and shouting out
Fainting spells, unsteadiness and falls
Frontotemporal dementia
Frontotemporal dementia can affect your motivation. (Getty Images)
Generally speaking, frontotemporal dementia is an uncommon type of dementia.While dementia generally mostly affects people over 65, this type typically starts at a younger age. Most cases are diagnosed in people aged 45-65, though it can also present in younger or older people.
Frontotemporal dementia affects the front and sides of the brain, and causes problems with behaviour and language. Similar to other types of dementia, it usually develops slowly and gets gradually worse over a long period of time.
Symptoms listed by the NHS include:
Personality and behaviour changes – acting inappropriately or impulsively, appearing selfish or unsympathetic, neglecting personal hygiene, overeating, or loss of motivation
Language problems – speaking slowly, struggling to make the right sounds when saying a word, getting words in the wrong order, or using words incorrectly
Problems with mental abilities – getting distracted easily, struggling with planning and organisation
Memory problems – these only tend to occur later on, unlike more common forms of dementia, such as Alzheimer’s disease
As well as mental symptoms, there may be physical ones too, such as slow or stiff movements, loss of bladder or bowel control, muscle weakness or difficulty swallowing. Frontotemporal dementia can also lead to someone being unable to care for themselves.
The first drug to slow the destruction of the brain in Alzheimer’s has been heralded as momentous.
The research breakthrough ends decades of failure and shows a new era of drugs to treat Alzheimer’s – the most common form of dementia – is possible.
Yet the medicine, lecanemab, has only a small effect and its impact on people’s daily lives is debated.
And the drug works in the early stages of the disease, so most would miss out without a revolution in spotting it.
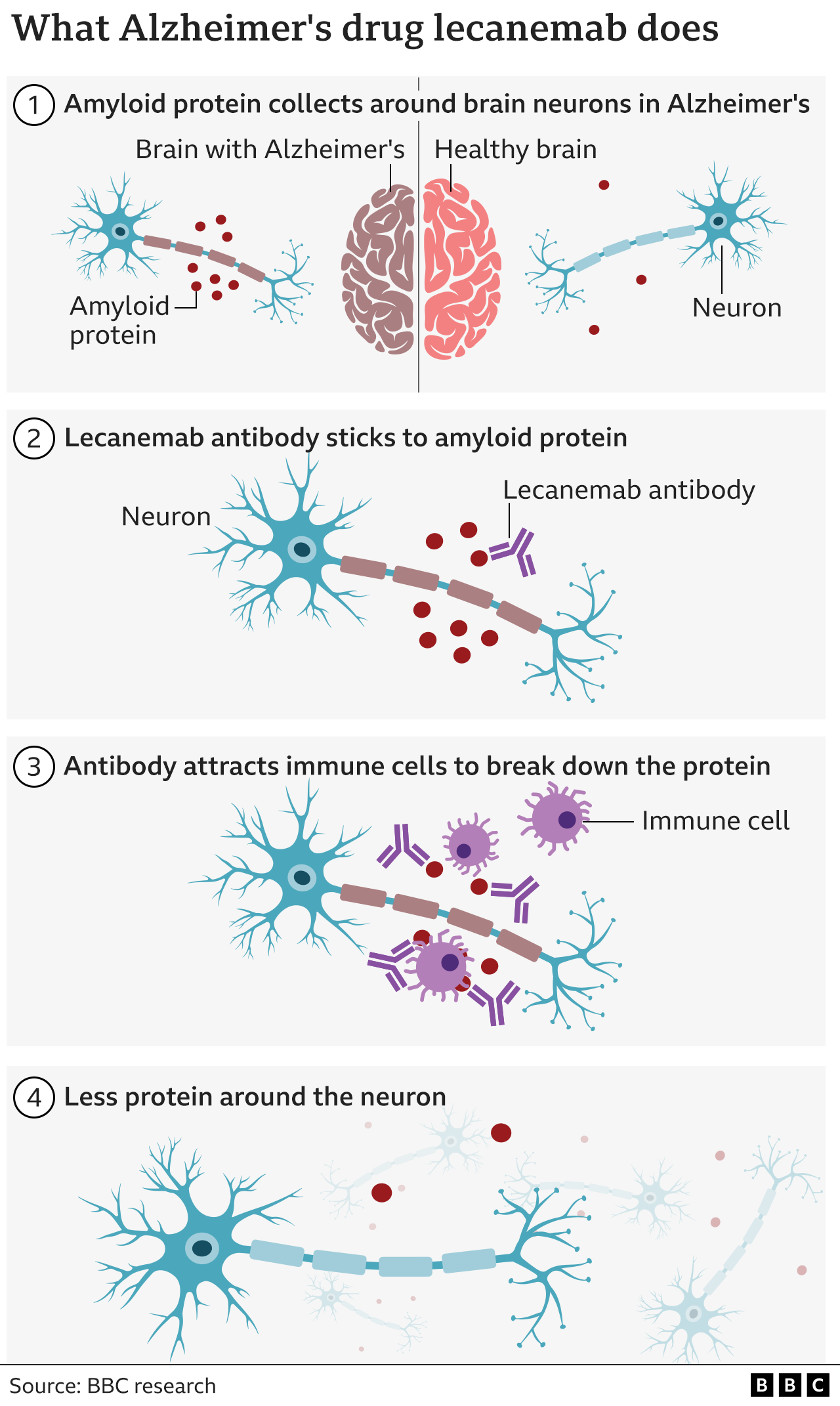
Lecanemab attacks the sticky gunge – called beta amyloid – that builds up in the brains of people with Alzheimer’s.
For a medical field littered with duds, despair and disappointment, some see these trial resultsas a triumphant turning point.
Alzheimer’s Research UK said the findings were “momentous”.
One of the world’s leading researchers behind the whole idea of targeting amyloid 30 years ago, Prof John Hardy, said it was “historic” and was optimistic “we’re seeing the beginning of Alzheimer’s therapies”. Prof Tara Spires-Jones, from the University of Edinburgh, said the results were “a big deal because we’ve had a 100% failure rate for a long time”.
Currently, people with Alzheimer’s are given other drugs to help manage their symptoms, but none change the course of the disease.
Lecanemab is an antibody – like those the body makes to attack viruses or bacteria – that has been engineered to tell the immune system to clear amyloid from the brain.
Amyloid is a protein that clumps together in the spaces between neurons in the brain and forms distinctive plaques that are one of the hallmarks of Alzheimer’s.
The large-scale trial involved 1,795 volunteers with early stage Alzheimer’s. Infusions of lecanemab were given every fortnight.
The results, presented at the Clinical Trials on Alzheimer’s Disease conference in San Francisco and published in the New England Journal of Medicine, are not a miracle cure. The disease continued to rob people of their brain power, but that decline was slowed by around a quarter over the course of the 18 months of treatment.
The data is already being assessed by regulators in the US who will soon decide whether lecanemab can be approved for wider use. The developers – the pharmaceutical companies Eisai and Biogen – plan to begin the approval process in other countries next year.
Image caption,
David Essam, with his wife Cheryl, has been taking part in the trial
David Essam, who is 78 and from Kent in the UK, took part in the international trial.
His Alzheimer’s meant he had to give up work as a joiner – he could no longer remember how to build a cabinet or use his tools. He now uses a digital watch as he can’t tell time using a clock face.
“He’s not the man he was, he needs help with most things, his memory in general is almost non-existent,” said his wife Cheryl. But she said the trial had given the family hope.
David said: “If somebody can slow it [Alzheimer’s] down and eventually stop it all together that would be brilliant, it’s just a horrible nasty thing.”
There are more than 55 million people in the world like David and the numbers with Alzheimer’s disease are projected to exceed 139 million by 2050.
Will it make a difference?
There is debate among scientists and doctors about the “real world” impact of lecanemab.
The slower decline with the drug was noticed using ratings of a person’s symptoms. It’s an 18-point scale, ranging from normal through to severe dementia. Those getting the drug were 0.45 points better off.
Prof Spires-Jones said that was a “small effect” on the disease, but “even though it is not dramatic, I would take it”.
Dr Susan Kohlhaas, from Alzheimer’s Research UK, said it was a “modest effect… but it gives us a little bit of a foothold” and the next generation of drugs would be better.
There are also risks. Brain scans showed a risk of brain bleeds (17% of participants) and brain swelling (13%). Overall, 7% of people given the drug had to stop because of side effects.
A crucial question is what happens after the 18 months of the trial, and the answers are still speculation.
Dr Elizabeth Coulthard, who treats patients at North Bristol NHS Trust, says that people have, on average, six years of living independently once mild cognitive impairment starts.
Slow that decline by a quarter and it could equate to an extra 19 months of independent life, “but we don’t know that yet”, she says.
It is even scientifically plausible that the effectiveness could be greater in longer trials. “I don’t think we can assume that this is it,” says Dr Kohlhass.
The emergence of drugs that do alter the course of the disease asks big questions of whether the health service is ready to use them.
The drugs have to be given early in the disease before too much damage to the brain is done, whereas most people referred to memory services are in the later stages of the disease.
That requires people coming forward at the earliest signs of memory problems and doctors being able to send them for amyloid tests – either brain scans or spinal fluid analysis – to a determine if they have Alzheimer’s or another form of dementia. At the moment only 1-2% of people with dementia have such tests.
“There’s an enormous gulf between current service provision and what we need to do, to deliver disease modifying therapies,” said Dr Coulthard.
She said that, currently, only those living near big medical centres or paying privately were likely to benefit.
Scientists also stressed that amyloid was only one part of the complex picture of Alzheimer’s disease and should not become the sole focus of therapies.
The immune system and inflammation are heavily involved in the disease and another toxic protein called tau is the one that’s found where brain cells are actually dying.
“That’s where I would put my money,” said Prof Spires-Jones.
She added: “I’m very excited we’re on the cusp of understanding enough to get a hold of the problem and we should have something that will make a bigger difference in a decade or so.”
A young woman says she’s now facing a dilemma after her much older boyfriend brought up the topic of marriage, casually asking her whether this would be something she’d be open to. According to the 23-year-old woman, she’s been with her ‘wonderful’ 71-year-old boyfriend for two years, and loves and cares for him very much.
At the moment, he’s in relatively good health and lives an active lifestyle. The longevity of his parents, who both lived until their nineties, has further reassured her that would have plenty of time together as a married couple. The potential bride-to-be doesn’t want children and feels as though their marriage could very well work out, however, she does have a few concerns about the caring role she may one day have to take on.
Taking to Reddit, where she goes by the username u/cinnamonpenguinss, the conflicted girlfriend wrote: “His mum does have Alzheimer’s or dementia, and is very frail. This leads me to believe that there will be a point in his life when he will need extra care.
“His dad did not have memory issues but did have a stroke. He doesn’t have any children, so I would be taking care of him as he gets older. What does it look like to care for an aging partner, especially if you have a job/career?
“It’s a little strange planning for an end of a marriage, but I fully believe that a decade or two of happiness with him is better than not. I just want to make sure that I am the right one to take care of him and love him.”
Opinions were mixed as to whether she should go ahead and marry her other half, with some even arguing she’d be ‘wasting the best years’ of her life.
One person urged: “You are signing up to be his nurse, not his wife. Don’t sabotage yourself like this! You deserve better. Don’t waste your young years being a servant. This is a horrible idea.
“This will damage you and set you back for the rest of your life, you must listen to the women who made the same mistake and are regretting it because of how the stress of being a 24/7 nurse and servant made them sick for the rest of their lives, to the point of needing but not affording someone to help them.”
Others however were more encouraging, with one sympathetic person, who sadly lost their much older husband to cancer, commenting: “I adored my husband. If I had the time again knowing I was going to lose him and there was nothing I could do about it. I would still do it all again.
“Even if you were with someone your own age there would still be a likelihood of one of you acting for the other further down the line anyway so take your happiness if you love them then it won’t be a barrier. It certainly wasn’t for me.”
A diagnosis of dementia more than doubles the risk of suicide in the first three months after a patient is told the news, according to the latest research.
The study, which followed nearly 600,000 English people for 18 years, found patients who already had a psychiatric condition, or who were younger than age 65 at the time of diagnosis, were at a similar risk. The risk was highest during the first three months after learning the news for people younger than 65: They were 6.5 times more likely to die by suicide.
“A dementia diagnosis can be devastating, but the immediate period after diagnosis is often the period of greatest distress,” said lead study author Dr. Charles Marshall, clinical senior lecturer and honorary consultant neurologist at the Wolfson Institute of Population Health at Queen Mary University of London.
“Receiving a diagnosis of Alzheimer’s at an early age is rare, unexpected and overwhelming, making it very difficult to accept,” said Beth Kallmyer, vice president of care and support for the Alzheimer’s Association, who was not involved in the study.
“One of the most important things you could tell someone facing an Alzheimer’s diagnosis is that they are not alone and support is available,” she said.
Prior research has established a distinct connection between dementia and suicide, including a 2021 study by Yale University scientists. “Adults over the age of 65 who were diagnosed with Alzheimer’s disease were twice as likely to die from suicide than older adults who did not suffer from dementia,” Kallmyer said.
Most cases of dementia are in the elderly, but chronic conditions and behavioral choices can play a role, according to Kallmyer. “Obesity, diabetes and sedentary lifestyles in younger people are rising quickly, and these are risk factors for dementia,” she said.
In the new study, published Monday in the journal JAMA Neurology, the actual number of people — 95 patients — who died by suicide after finding out they had dementia was small. However, that did not diminish the study’s value in identifying the most vulnerable subgroups and three-month timing, Marshall said.
Past studies have also found a relationship between a diagnosis of dementia and suicide in people diagnosed at an earlier age. While the new study was unable to determine why this would be so, Marshall pointed to the interpersonal theory of suicide as a possible answer.
“Perceived burdensomeness is a critical pillar for suicidal behavior,” Marshall said. “That perception of burdensomeness may be higher in younger patients with dementia who are more likely to be in their work-productive years as well as have family-caring responsibilities.”
Results from studies like these suggest that physicians should conduct a “robust risk assessment” for signs of suicide at the time of diagnosis, Marshall and his coauthors wrote in the latest study.
“We know that early Alzheimer’s disease can cause low mood, anxiety and social isolation. These symptoms might be both causes and signs of suicide risk,” Marshall said in an email.
Becoming educated about dementia “and in particular, younger onset Alzheimer’s disease, is an important first step in supporting someone who receives a younger onset diagnosis,” Kallmyer said.
Health and financial plans should be put in place early so that the person living with dementia can participate in those decisions, she suggested.
“If the person is still working, it’s critical that they investigate employment benefits that could help them — and it’s essential that they do this before they leave their jobs. Employer benefits might include short- and long-term disability insurance, which can be very helpful while they are applying for Social Security disability,” Kallmyer said.
Signs of depression and suicidal warning signs mimic those of dementia, making it extremely difficult for caregivers, according to the Alzheimer’s Association.
“Because of the complexities involved with diagnosing depression with dementia, it may be helpful to consult a geriatric psychiatrist who specializes in recognizing, diagnosing, and treating depression in older adults,” the association noted.
The US Substance Abuse and Mental Health Services Administration, or SAMHSA, has developed a series of resources for caregivers. If you or a loved one needs suicide or mental health-related crisis support, SAMHSA encourages calls or texts to the 988 suicide and crisis lifeline. There is also a tool to find providers of treatment and support.
Want to reduce your risk for dementia? Slap on a step counter and start tallying your steps — you’ll need between 3,800 and 9,800 each day to reduce your risk of mental decline, according to a new study.
People between the ages of 40 and 79 who took 9,826 steps per day were 50% less likely to develop dementia within seven years, the study found. Furthermore, peoplewho walked with “purpose” — at a pace over 40 steps a minute — were able to cut their risk of dementia by 57% with just 6,315 steps a day.
“It is a brisk walking activity, like a power walk,” said study coauthor Borja del Pozo Cruz, an adjunct associate professor at the University of Southern Denmark in Odense, Denmark, and senior researcher in health sciences for the University of Cadiz in Spain.
Even people who walked approximately 3,800 steps a day at any speed cut their risk of dementia by 25%, the study found.
“That would be enough, at first, for sedentary individuals,” said del Pozo Cruz in an email.
“In fact, it is a message that doctors could use to motivate very sedentary older adults — 4k steps is very doable by many, even those that are less fit or do not feel very motivated,” he added. “Perhaps, more active and fitter individuals should aim for 10k, where we see maximum effects.”
But there was a even more interesting result buried in the study, according to an editorial entitled “Is 112 the New 10,000?” published Tuesday in JAMA Neurology.
The largest reduction in dementia risk — 62% — was achieved by people who walked at a very brisk pace of 112 steps per minute for 30 minutes a day, the study found. Prior research has labeled 100 steps a minute (2.7 miles per hour) as a “brisk” or moderate level of intensity.
The editorial argued that individuals looking to reduce their risk of dementia focus on their walking pace over their walked distance.
“While 112 steps/min is a rather brisk cadence, ‘112’ is conceivably a much more tractable and less intimidating number for most individuals than ‘10,000,’ especially if they have been physically inactive or underactive,” wrote Alzheimer’s researchers Ozioma Okonkwo and Elizabeth Planalp in the editorial. Okonkwo is an associate professor in the department of medicine at the Wisconsin Alzheimer’s Disease Research Center at the University of Wisconsin–Madison; Planalp is a research scientist in Okonkwo’s lab.
“We do agree this is a very interesting finding,” said del Pozo Cruz via email. “Our take is that intensity of stepping matters! Over and above volume. Technologycould be use to track not only number of steps but also pace and so these types of metrics can also be incorporated in commercial watches. More research is needed on this.”
Don’t have a step counter? You can count the number of steps you take in 10 seconds and then multiply it by six — or the number of steps you take in six seconds and multiply it by 10. Either way works. But remember, not everyone’s steps are the same length, nor are their fitness levels. What might be a brisk pace for a 40-year-old may not be sustainable for a 70-year-old.
Editor’s Note: Before beginning any new exercise program, consult your doctor. Stop immediately if you experience pain.
Inside the study
The study, also published Tuesday in JAMA Neurology, analyzed data from over 78,000 people between the ages of 40 and 79 who wore wrist accelerometers. Researchers counted each person’s total number of steps per day, and then placed them into two categories: Fewer than 40 steps per minute — which is more of an amble, like when you’re walking from room to room — and more than 40 steps per minute, or so-called “purposeful” walking. The researchers also analyzed peak performers — those who took the most steps within 30 minutes over the course of a day (although those 30 minutes did not have to occur on the same walk).
Researchers then compared that person’s steps against their diagnosis of dementia of any type seven years later. After controlling for age, ethnicity, education, sex, socio-emotional status and how many days they wore an accelerometer, researchers also factored out such lifestyle variables as poor diet, smoking, alcohol use, medication use, sleep issues and a history of cardiovascular disease.
The study did have some limitations, its authors point out — it was only observational, so it cannot establish a direct cause and effect between walking and a lower risk of dementia. In addition, “the age range of participants may have resulted in limited dementia cases, meaning our results may not be generalizable to older populations,” the study said.
“Because there are often considerable delays in dementia diagnosis, and this study did not include formal clinical and cognitive assessments of dementia, it is possible that the prevalence of dementia in the community was much higher,” the authors added.
While agreeing that the findings cannot be interpreted as a direct cause and effect, “the mounting evidence in support of the benefits of physical activity for maintaining optimal brain health can no longer be disregarded,” wrote Okonkwo and Planalp.
“It is time for the management of physical inactivity to be considered an intrinsic part of routine primary care visits for older adults,” they added.
Research adds up
Indeed, recent research published in July has found many leisure activities, such as household chores, exercise, adult education classes and visiting with family and friends, affected dementia risk in middle-aged people.
Adults who were highly engaged in physical activity such as frequent exercise had a 35% lower risk of developing dementia compared with people who were the least engaged in these activities, researchers found.
Regularly doing household chores lowered risk by 21% while daily visits with family and friends lowered the risk of dementia by 15%, when compared with people who were less engaged.
Everyone in the study benefited from the protective effect of physical and mental activities, whether or not they had a family history of dementia, researchers found.
Another study published in January found that exercise may slow dementia in active older people whose brains already showed signs of plaques, tangles and other hallmarks of Alzheimer’s and other cognitive diseases.
That study found exercise boosts levels of a protein known to strengthen communication between brain cells via synapses, which may be a key factor in keeping dementia at bay.
“Dementia is preventable to a great extent,” said del Pozo Cruz. “Physical activity as well as other lifestyle behaviors such lack of alcohol and smoking, maintaining a healthy diet and weight and sleep can put you on the right track to avoid dementia.”
Namibia, AfricaRelatives of Ndikuhoole Johanna Nakamhela began noticing the changes eight years ago when she struggled to recall significant moments in her life. She also seemed anxious when mingling with members of her church, something she’d done easily in her decades as a minister’s wife. These changes weren’t typical of the normal aging process, her doctor said, and a brain scan confirmed as much.
Now, when the 77-year-old Nakamhela potters in her kitchen at home in Kalkfeld, a small town just north of the Namibian capital, a caregiver hovers nearby to ensure that she doesn’t leave a pot unattended on the stove or get into trouble with an open gas flame. Her changing brain state often seems to trap her in a private inner world. But other times, her body language indicates she’s content, even when words fail her.
Nakamhela is one of almost 7,700 Namibians living with dementia in a population of 2.5 million. Across southern Africa, nearly 300,000 people were estimated to suffer from dementia in 2019, according to the The Lancet Public Health journal. As this population grows, and as gains in healthcare enable people to live longer, dementia in the region is expected to rise by 185 percent by mid-century, reaching around 830,000 cases by 2050.
Care for older people in Africa usually falls to families, with informal kinship networks serving as one of the primary ways to look after the aging population. But these traditional care and support systems are unraveling, even as people live longer and the number of older people with degenerative brain diseases swells. This raises questions about how communities will properly care for their elders if state social services don’t step in.
“Modern life has eroded that [traditional care],” says Phazisa Mbilini, a social worker from the South Africa-based non-profit Dementia SA. “With people getting more westernized, they think they’re living for themselves and not for other people.”
The Nakamhela family remains tight-knit, despite experiencing some of the same shifts reshaping the social geology of the subcontinent: urbanization, modernization, migration. The couple’s children—two lawyers, a chef-turned-journalist, and a tour guide—are now supporting their mother in her dotage.
By early 2021, she needed a daytime caregiver at home. Her husband Ngeno-Zacharias, also 77, a retired pastor, couldn’t stretch his pension far enough to cover this cost, so two of their sons are paying for the extra care. Another returned from South Africa to live with his parents to help with their needs.
The Nakamhela family is doing what many dementia experts recommend: When possible, rather than move their loved one into a private or state-run facility, allow the person to live in the familiarity and security of their own home or community.
Degenerative brain diseases
Dementia is the catch-all term for a range of slow-burning brain diseases that have similar symptoms: the incremental fading of a person’s memories and their ability to think and reason; changes in personality or behavior; and sometimes a loss of language or analytical skills. Alzheimer’s is the most common form of dementia, according to the Alzeihmer’s Association, based in Chicago, Illinois. Other degenerative brain diseases include vascular dementia, Lewy Body dementia, and frontotemporal dementia.
One of the hurdles to detecting these diseases early and starting treatment is that many doctors and nurses might misread these symptoms as signs of normal aging, says Karen Borochowitz, founder and director of Dementia SA. A 2019 Alzheimer’s Disease International report confirms this, finding that 62 percent of healthcare practitioners globally see dementia symptoms as run-of-the-mill aging.
Another factor that slows detection in Africa is the shortage of skilled medical specialists such as geriatricians, and the inaccessibility of expensive diagnostic brain scan technology, according to Borochowitz.
Kahimbi Mushanana is one of the many southern Africans who has not received a formal dementia diagnosis for these very reasons. The 82-year-old lives in a village 620 miles northeast of the Nakamhela home.
Mushanana’s son, Irvine, first noticed something was amiss in 2017 when his mother began repeating herself, looping through the same morning greetings or asking questions about things she should have known. Once, when she didn’t return from a routine trip to town, he found her lost on its once-familiar streets.
Doctors dismissed her faltering memory and disorientation as ordinary aging, but her son had an instinct that there was more to it than the simple misfiring of an octogenarian brain. Researching the symptoms online, he narrowed things down to descriptions of dementia. Even without a formal diagnosis, this knowledge has allowed the Mushanana family to understand the progression of the suspected disease, how to manage the 82-year-old’s changing behaviors, and adapt the home environment to keep her safe while also remaining socially connected.
Living with dementia
One spring morning in 2021, Nakamhela pored over an old photograph with her husband at her side. Whether her brain made connections to what she was seeing was unclear: Did she recall that the younger man in the picture is the pastor she married half a century earlier? Did she know that the child in the monochrome photograph, wearing a shirt and suspenders, is one of her four now-adult sons?
Living with dementia can be bewildering, both for the person living with the condition, as well as those close to them. Many of the person’s behaviors might be seen as “problematic,” explains Allen Power, a geriatrician with Canada’s University of Waterloo Research Institute for Aging. This highlights the need for education and outreach for family members like those of Nakamhela and Mushanana, he says.
Those closest to a person with dementia report struggling with how to communicate when a loved one can no longer find words to express themselves. Some may need to accept that their loved ones can’t recognize a spouse of 50 years or their grown children. How do they protect someone if they wander off into once-familiar territory and can’t find their way home again? They may need to manage distressing departures from reality or fantastical, aggressive rants or volcanic language from someone who seldom cursed. They might need to restructure their lives to keep someone safe when ordinary kitchen activities become dangerously unfamiliar. They have to learn to cope with physical aggression or lapses in hygiene.
Power explains that each individual’s experience of dementia will be unique, shaped by their own abilities, environment, and the progression of their degenerative disease. Viewing these symptoms as a disability rather than a disease can help home caregivers work around the sometimes confounding reactions.
“Many of the problem behaviors might be an attempt to communicate,” says Power.
“If someone starts hitting in the shower, they might be trying to tell you that the water is too cold. What in the environment needs to change, in response to the person’s attempt to communicate when they no longer have language?”
Since Getrud Kangandi began caring for Nakamhela early in 2021, the 35-year-old has grown to know her client well. Even though Nakamhela can’t express her needs, Kangandi knows she likes to wander through the family vegetable garden, and will stroll along with her to help her find the way. Allowing a person to keep doing what has always given them joy is important to their well-being, says Power.
Consistency of care is also key as a person’s dementia progresses, explains Power. The better a caregiver knows the person in their charge, the more they will understand their non-verbal communications.
Educating the public, families, and caregivers
Education can help destigmatize symptoms tied to dementia, as well as change how society views what is often seen as a “slow motion disaster,” according to mental health experts. Even the most sympathetic voices tend to use demeaning terminology in dementia narratives, describing someone as “lost” to their family, and their dementia as a “long death” while a person “fades away.”
“This may feel true for those nearest to the person,” Power says, “but this assumes that a person living with dementia is a passive recipient of care, forgetting that they are still active agents in their own lives and can still participate in the world around them.”
Burnout is one of the biggest difficulties facing at-home caregivers, according to Dementia SA’s Phazisa Mbilini, particularly when the burden falls on a single individual, usually a spouse, sibling, or adult child.
“Caring for someone living with dementia is a 24-7 thing,” she says. “Often, a person with dementia won’t sleep, or they might wake up during the night and want to wash curtains, or go to town.”
When engaged with education and outreach, Mbilini often encounters caregivers who believe they can’t leave the house or do anything else, because they need to stay with their loved one at all times.
“We try to advise the carer that they must allow other people to help them and give themselves time to go out and engage with others,” she says. “They mustn’t be ashamed to say they’re exhausted.”
One family’s care circle
As Mushanana’s dementia advances, the world around her remains relatively constant and her family has adapted to her changing needs. She lives with her extended family in a cluster of rustic wattle-and-daub homes, deep in the dry Namibian countryside, with no running water or electricity. The family cooks over an open outdoor fire. Her daughter Eunice is her primary day-to-day caregiver. Her son Irvine, who lives and works in nearby Katima Mulila, provides financial support and visits regularly.
As she ages, Mushanana requires help with bathing, dressing, and other basic needs. She can’t tend the cooking fire anymore and needs supervision during the day, since she loves to wander off into the nearby croplands where the family grows some of their food. Three of her granddaughters sleep in her two-room home so they can keep an eye on her at night.
The family lives far from the better-resourced cities, which might have care agencies that supply skilled or semi-skilled care staff. But these options are too expensive for most families, explains Borochowitz of Dementia SA. Most of those providing care in the region are domestic workers who may have rudimentary training in caring for the aging. Few have formal training for working with a person living with dementia, according to Dementia SA.
With the lack of trained caregivers or access to private or state-run outpatient support or residential care facilities, non-profit organizations have become critical to help families and communities access information and support, says Mbilini, who offers much of Dementia SA’s training and outreach programs in South Africa. These are particularly important forms of support for single-caregiver situations.
Around the world, the burden of caring for children and the elderly—the so-called “second shift”—falls largely to women who are often unpaid. The World Health Organization’s 2021 Global Status Report on the Public Health Response to Dementia estimates that 70 percent of this kind of dementia care is done by women.
“In 2019, informal dementia carers spent over 89 billion hours providing support with activities of daily living (ADLs)—about 5 hours per day per person with dementia. Informal care provision… is particularly high in countries with low resources where there is a scarcity or lack of formal support services for dementia,” says the report.
Civil society organizations such as the social justice-focused think tank Institute for Economic Justice in South Africa suggest that extending social welfare grants or even instituting a universal basic income grant can support family members who do this kind of unpaid care work.
But in a setting as rural and traditional as Mushanana’s, her changing state of mind does not seem to disrupt the family’s normal day. One morning she took a seat on the sandy ground amid the cluster of thatched family homes. She chattered away contentedly, to no one in particular, and chuckled, clapping her hands in mirth. Then maternal instincts kicked in as a toddler nearby cried in distress. Mushanana reached for the child, drawing the whimpering girl onto her lap for comfort.
Grandmother and great-granddaughter sat in wordless communion while the rest of the family went about their day.
Showing love and acceptance to their aging matriarch is central to her wellbeing, says Irvine: “We must understand and accept that this is how she is now.”
Lee-Ann Olwage is a visual storyteller from South Africa who uses collaborative storytelling to explore themes relating to gender and identity.
South African science writer Leonie Joubert’s books include Scorched, Boiling Point, and The Hungry Season.
The Premier League has written to its clubs to tell them they are considering whether to ban some academy players from heading a football amid dementia fears.
According to British media reports on Wednesday, Premier League chiefs have emailed all 20 top-flight teams in the wake of a recent study into the link between football and dementia.
Last week, a report published and titled ‘Football’s Influence on Lifelong Health and Dementia Risk’ found footballers were three-and-a-half times more likely to suffer from degenerative brain conditions than the general population.
The research looked at 7,676 Scottish footballers born between 1900 and 1976 who were matched with 23,000 people from similar areas and backgrounds.
It led to the Scottish Football Association considering a ban on children under 12 heading the ball and former player Lenny Johnrose, who was diagnosed with motor neurone disease in March 2017, called for children aged 14 and under to be banned from heading.
The United States is the only country in the world which has a similar ban. Children aged 10 and under are not allowed to head the ball in games or practice, while there are limits placed in training sessions for 11-to-13 year olds.
In the wake of the study, led by consultant neuropathologist Dr Willie Stewart of Glasgow University, Premier League interim chief executive Richard Masters is looking into the latest findings to decide if any age groups should be banned from heading.
The FA’s independently chaired medical and football advisory group does not yet believe there is enough evidence at this stage to make changes to the way modern-day football is played, at any level of the game.
It has reissued best practice coaching advice in youth football, which advises limiting repetitive heading practice and using age-appropriate balls and softer items like balloons or sponge balls.